

Surgical staff traditionally track patients as they move through the surgical process on a large, centrally located whiteboard. Although whiteboards are low-tech, they provide the advantage of being easy-to-use and understand, and can never go down and lock the user out of their information (unless a staff member erases something!).
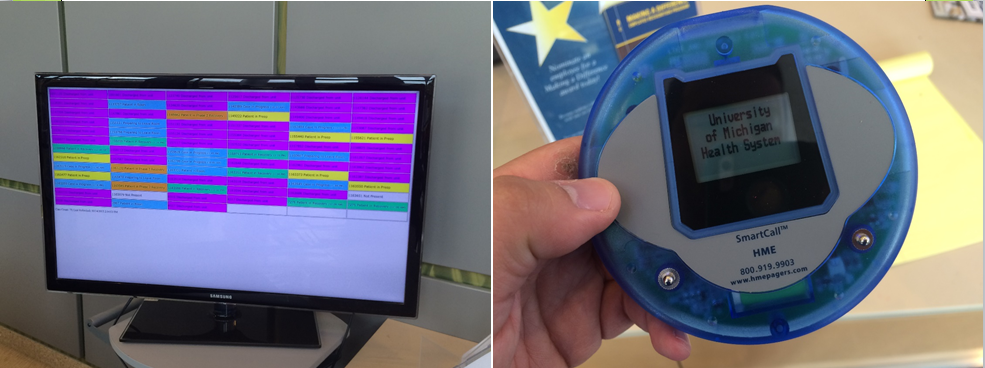
Over the years most departments have begun to move to "digital whiteboards" for tracking surgical patients. Some of these programs can be edited by working directly off of a large touch screen that take the place of a whiteboard, but most are programs which allow for manual and automated tracking of patients as they are checked into different departments. One or two central clerks usually maintain this information, with a tracking dashboard showing in several different locations on large monitors.
Digital whiteboards, or digital surgical patient trackers, have the advantage of allowing surgeons and anesthetists to check on the progress operating rooms remotely so they can plan when to get ready for their cases more efficiently (instead of calling surgical departments). They also allow departments downstream in patient receiving to anticipate patient volume in real-time.
In this project, I collaborated with a team of analysts and consultants and lead the evaluation of a digital surgical tracker being used at several major hospitals across the United States. I identified weaknesses in the current product through usability testing, observations, and stakeholder interviews. Then, I redesigned the product through a series of iterative collaborative designs and rapid usability testing with paper prototypes. Finally, I worked with a development team to generate functional stories based on personas and scenarios for the development process.
The end result was a greatly improved surgical tracker which allowed display customization by department, remote access of patient status by surgical staff, and provided a waiting-room-facing component which allowed family members to track their loved-one's progress and decrease concerned phone calls to surgery.
Photo Credit: Army Medicine
Through early usability testing, I quickly discovered that surgical staff found their patient tracker software, confusing and unusable.
A large part of this problem came from a mismatch between user's mental model of how they previously tracked patients and the format that the software displayed patient information.
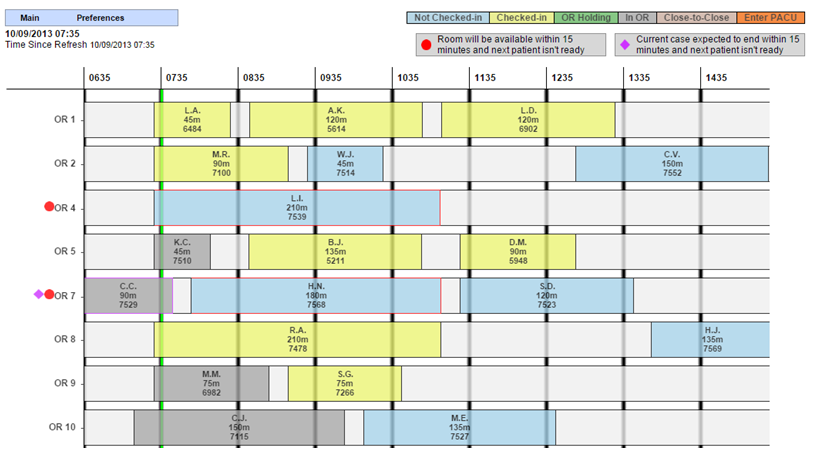
Whiteboards tracking patients are usually composed of rows of patient names with symbols indicated in marker or magnets signalling a patient's progression. However, their tracking software provided a visual time span for each patient in a rectangular block which moved across the screen with the progression of time.
This mismatch in expectations moved users to revert back to their old tracking habits as they abandoned the product. Users who no longer had whiteboards to revert to, created Excel sheets which they mocked-up like whiteboards.
This gave me an early indication of user preferences, mental models, and use patterns, and would provide design ideas for me later in the process.
Before starting on a redesign, I visited several hospitals to see how their surgical patient trackers functioned. In addition to convergence in many design areas, many commercial trackers employed a patient facing system that allowed family members to track the progress of their loved-ones in surgery. This helped to decrease the anxiety of those in the waiting rooms and decreased calls to the main desk asking about patient status'.
I noted this patient-family facing component as a clear need in our redesign.
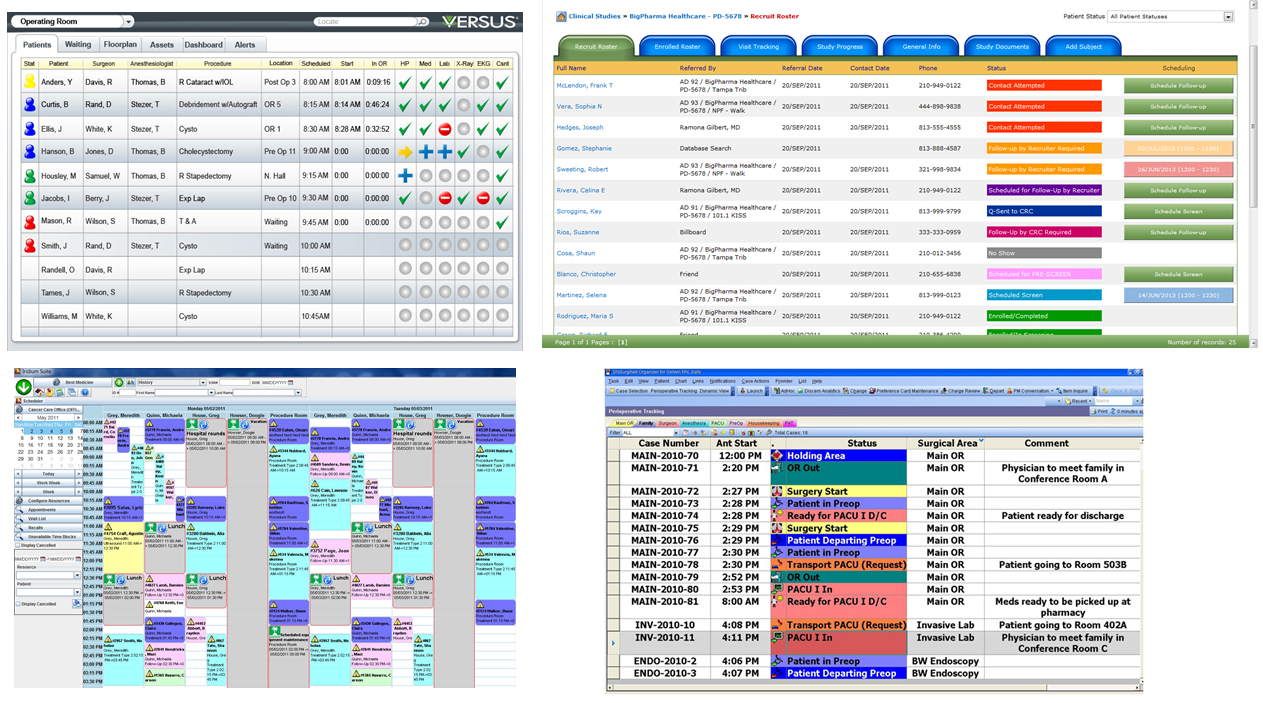
In addition to visiting sites and observing the use of surgical software in the wild, I researched surgical tracking software to compare design patterns. I read commentary from physicians detailing features they liked (or hated) and generated notes on some of the basic elements which would be necessary in the redesigned tracker.
Throughout this process, I interviewed many surgeons, anesthesiologists, techs, and clerks to discover their needs and preferences for a surgical tracker.
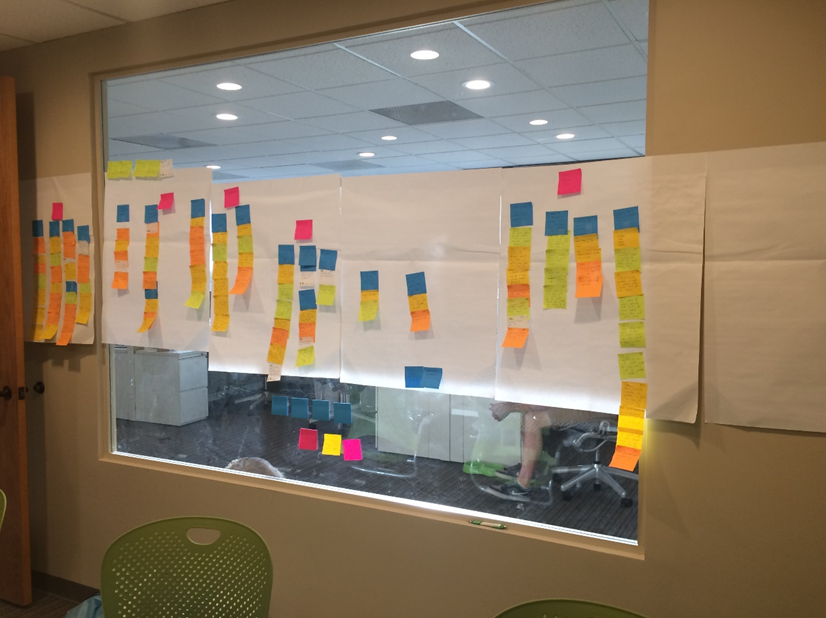
After compiling these notes, I worked with a team to extract the most important themes and quotes and wrote them on sticky notes. Then I lead an affinity diagramming session in which we grouped items with similar themes and then created super groups of those themes.
I prefer using affinity diagramming for qualitative coding when I have a group of analysts because it allows us to use our collective brainpower to determine thematic categories, democratizes the interpretation of the data (no one person is doing it), and allows the data to "speak for itself" in forming organic themes.
The high-level themes from this exercise would help target the needs and wants that the tool should satisfy.
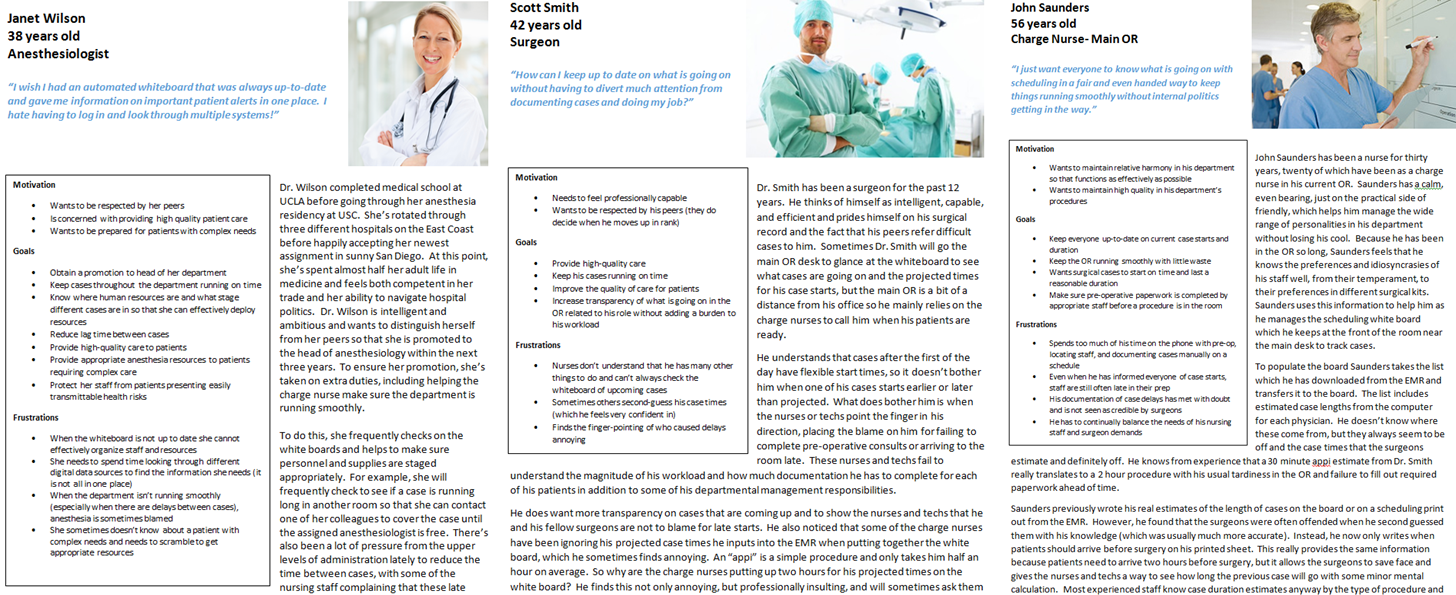
Utilizing the notes which I had taken during my site visits, I created personas and scenarios, noting the motivations, goals, and frustrations of our primary and secondary user groups.
These personas and scenarios, in conjunction with the affinity diagram would help to bound our design efforts and keep us focused on the needs of our users.
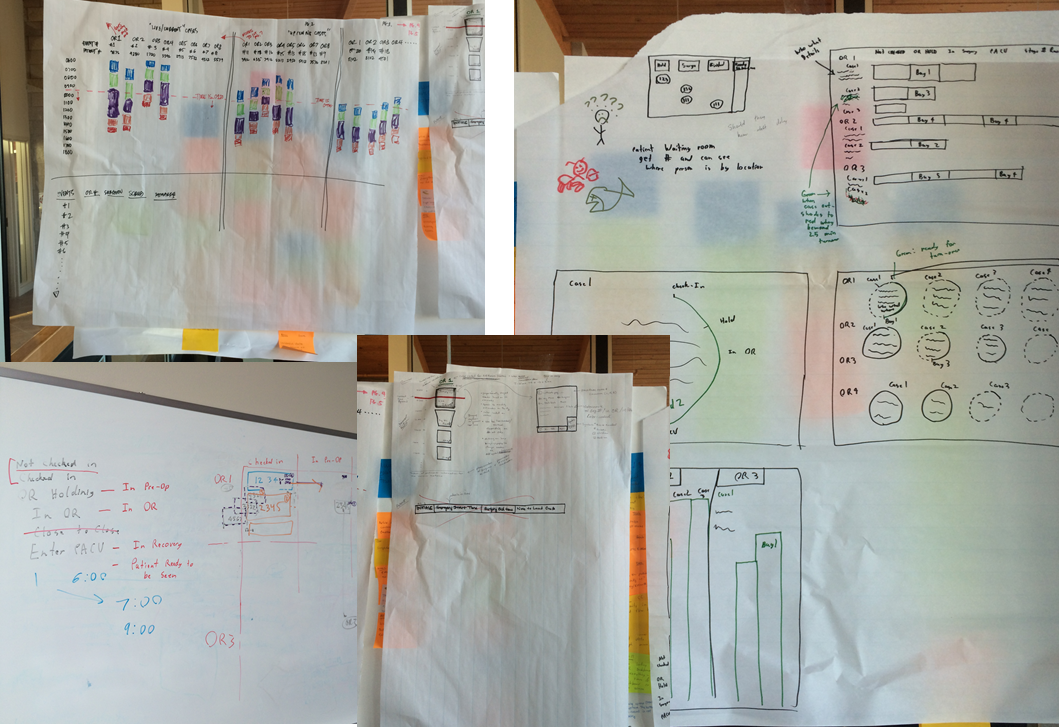
With the information we had collected, I led the team in a week of collaborative design, sketching, and idealization for potential redesigns.
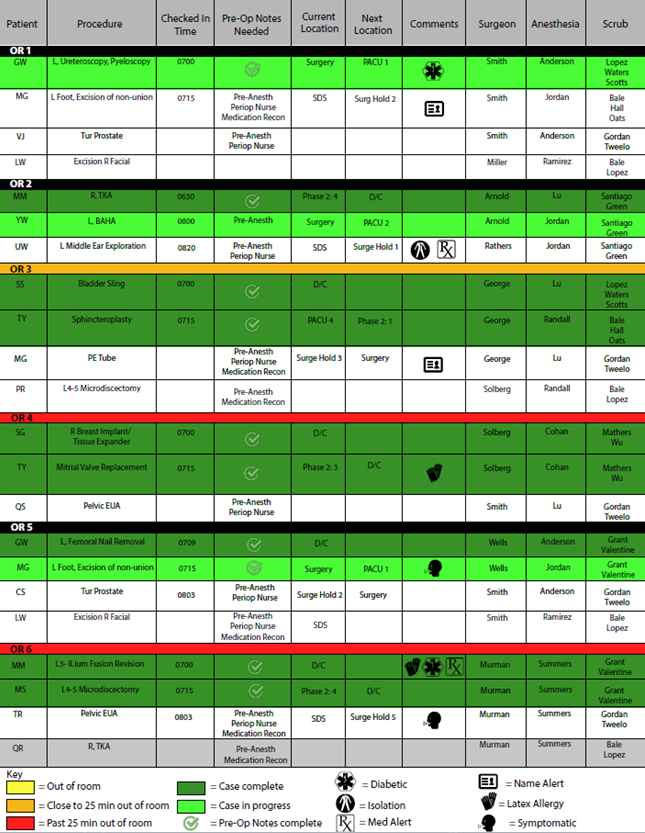
After the ideation sessions, I created my first attempt of redesigning the digital surgical tracker using Illustrator. This early version was an attempt to take best practices in surgical tracker design across the industry and meld it with the ease and familiarity of the whiteboard/Excel sheets that the staff was accustomed to using.
NOTE: All names on mock-ups are fictional and do not represent real patients.
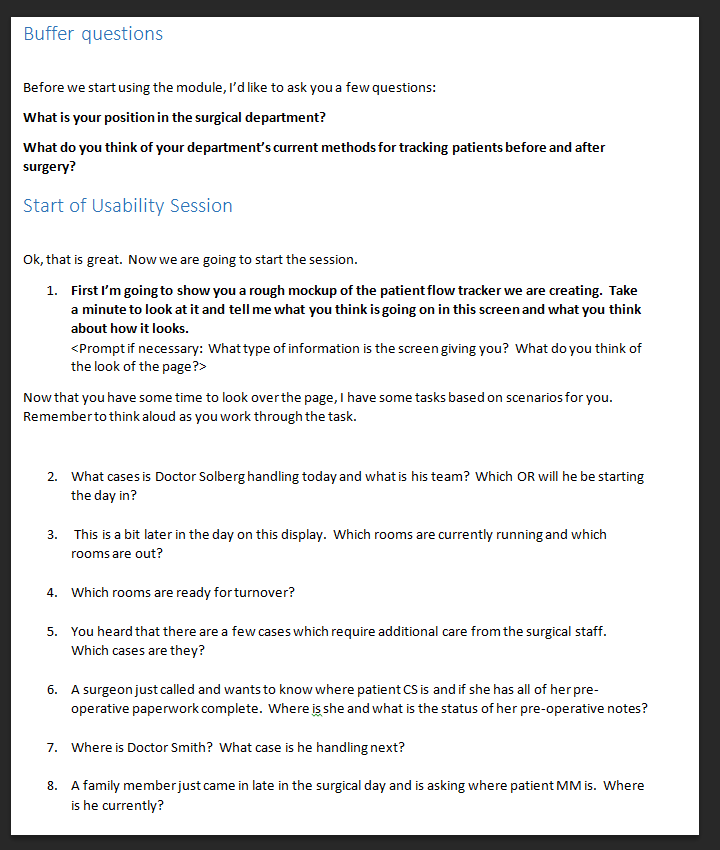
I conducted usability tests on our early designs as paper prototypes, in which I had several different sheets to simulate patient movement throughout the day.
We quickly learned that we needed to reduce the number of colors on the screen and simplify elements of the interface. However, our most significant discovery was related to accessibility: A large portion of our users were colorblind.
This meant that the color codes of green red, and yellow were indistinguishable and that many users could not tell if a case was finished or in progress in this design.
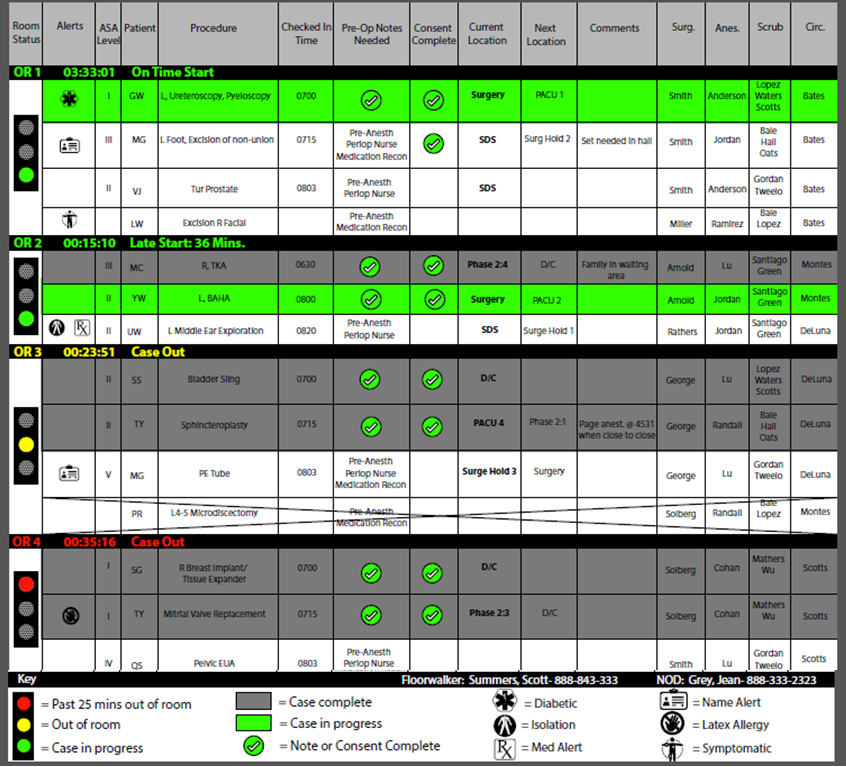
Our client liked the idea of green, yellow, and red signaling when surgical rooms were out. This presented a moderate design problem, because purely signaling room information with these colors would render the tool unusable for colorblind staff. As a compromise, we created positional signaling and color signaling to communicate surgical room status.
The positional signaling was provided by using a traffic light for each room. When the bottom circle was lit, the room was in session, and when either of the top two circles were lit the room was out. Color was preserved in the color of the traffic lights and by highlighting in-session rooms with a lighter green that contrasted with the grayed out completed rooms. We also added textual cues, stating when cases were out, to further alert users to the room status.
After several rounds of usability testing this design was tweaked until both colorblind and non-color blind users found it satisfactory.
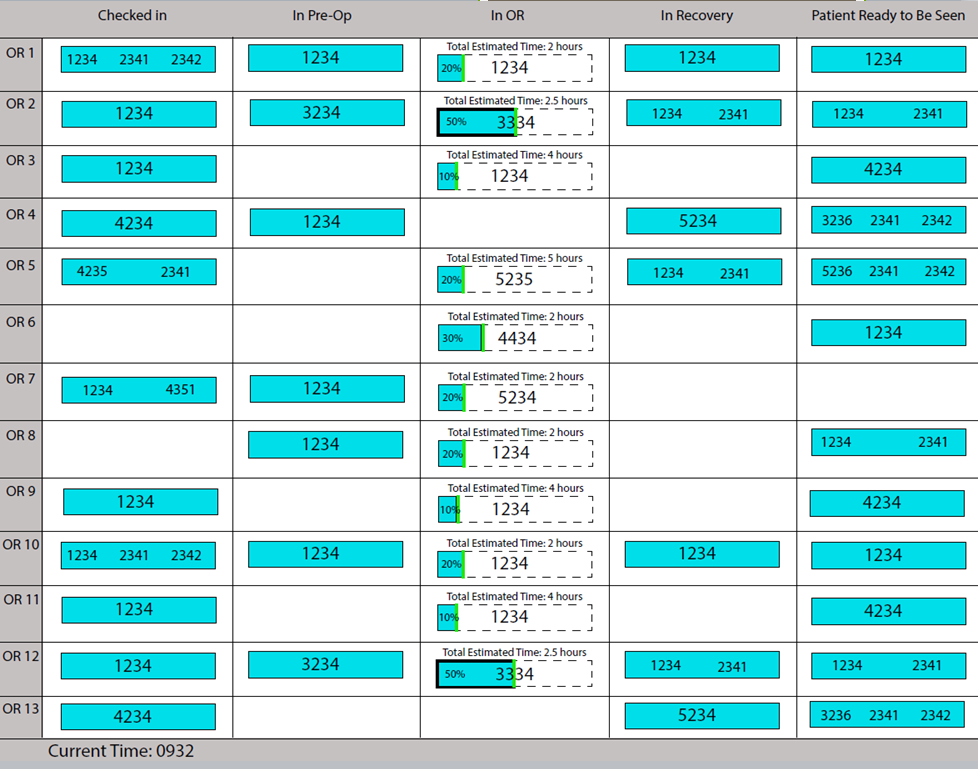
In addition to the surgical staff-facing tracker, I worked with the team to design and usability test several versions of a waiting-room tracker for family members. In the patient-family facing tracker, patients are represented by numbers which family receive on a sheet when the patient is admitted. The location of the patient in the surgical process is indicated by the column they are in.
Users found several patient numbers in the same box confusing. Interestingly, many users did not like to see the progression of their loved one while they were in the surgical room itself. This seemed to provoke fear and anxiety as users expressed dismay at the thought of the details of the procedure.
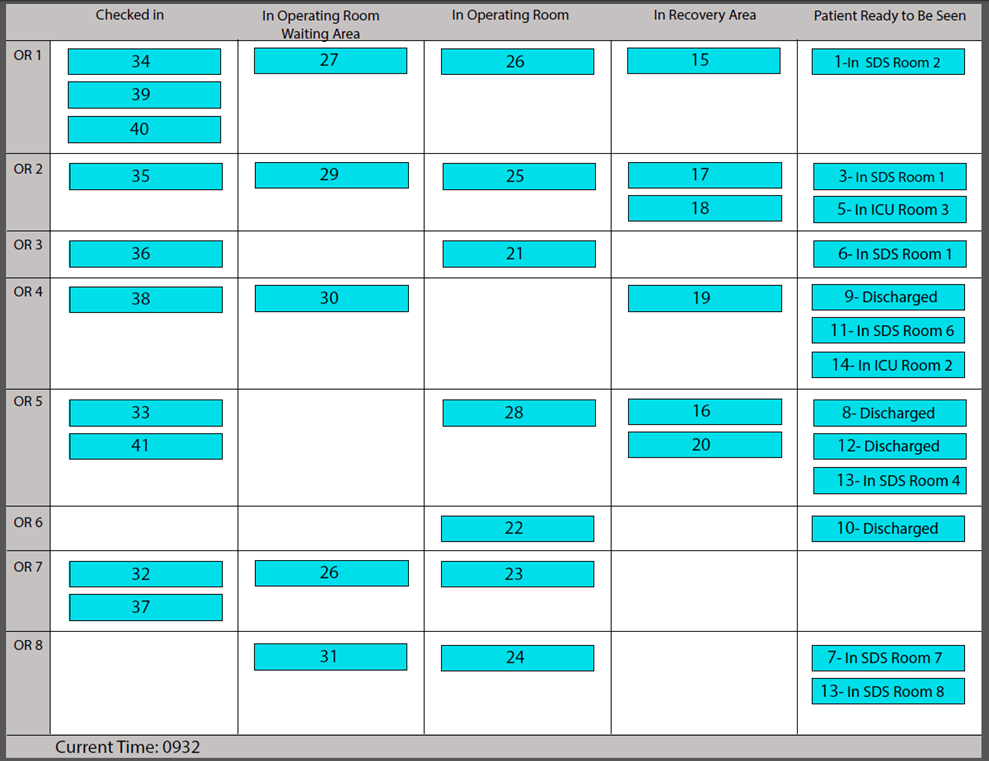
In the final patient-family facing tracker, only one number is represented in each square to reduce confusion, and the progression of surgery while the patient is in the operation room is not represented to avoid family-member discomfort.
Digital Surgery Tracker
Surgical staff traditionally track patients as they move through the surgical process on a large, centrally located whiteboard. Although whiteboards are low-tech, they provide the advantage of being easy-to-use and understand, and can never go down and lock the user out of their information (unless a staff member erases something!).
Over the years most departments have begun to move to "digital whiteboards" for tracking surgical patients. Some of these programs can be edited by working directly off of a large touch screen that take the place of a whiteboard, but most are programs which allow for manual and automated tracking of patients as they are checked into different departments. One or two central clerks usually maintain this information, with a tracking dashboard showing in several different locations on large monitors.
Digital whiteboards, or digital surgical patient trackers, have the advantage of allowing surgeons and anesthetists to check on the progress operating rooms remotely, so they can plan when to get ready for their cases more efficiently (instead of calling surgical departments). They also allow departments downstream in patient receiving to anticipate patient volume in real-time.
In this project, I collaborated with a team of analysts and consultants and lead the evaluation of a digital surgical tracker being used at several major hospitals across the United States. I identified weaknesses in the current product through usability testing, observations, and stakeholder interviews. Then I redesigned the product through a series of iterative collaborative designs and rapid usability testing with paper prototypes. Finally, I worked with a development team to generate functional stories based on personas and scenarios for the development process.
The end result was a greatly improved surgical tracker which allowed display customization by department, remote access of patient status by surgical staff, and provided a waiting-room-facing component which allowed family members to track their loved-one's progress and decrease concerned phone calls to surgery.




























